Surgical resection is the standard of care for localised gastric cancer. In Indian subcontinent majority of patients with gastric cancer present in nonsurgical stage, as comapred to the japanese counterpart, because of routine screening and surveillence. In general oncologic goal is to achieve micro and macroscopically complete resection (R0 resection)
Three issues are important when considering for surgical resection of gastric cancer.
The extent of gastric resection depends upon the location of tumour and surgical margins. A general oncological consensus has been formed that, a 5cm grossly negative margin around the tumour and microscopically negative margins (R0) are the treatment goals. We at Dharamshila Hospital, prefer frozen section analysis of the proximal and distal margins to know the completeness of resection. For the mid and distal gastric cancer, subtotal and distal partial gatrectomy suffice. For the proximal gastric cancer, either total gastrectomy or oesophagogastrectomy through combined abdominal and thoracic approach is suitable. The aim should be oncologically sound resection with microscopic negative margin.
D1 dissection – Limited lymphadenectomy of perigastric lymph nodes
D2 dissection – En bloc removal of second echelon lymph nodes with tail of pancreas and spleen
Modified D2 dissection – D2 dissection sparing pancreas and spleen
The idea behind doing lymphadenectomy involves two important issues.
Staging– Removal and histopathological analysis of adequate number of lymph nodes.
Therapeutic– Some form of lymphadenectomy may be therapeutic.
The current AJCC staging system suggests analysis of atleast 16 lymphnodes or more to assign a pathologic N stage.
To achieve this goal– Surgeons must perform adequate lymphadenectomy and the pathologists must retrieve and examine at least 16 lymphnodes to provide optimal pathologic staging.
Moreover, the concept of RML (Ratio of metastatic lymph node) has come up, which signifies and determines the prognosis of the case depending on the number of positive lymph nodes, out of total lymph nodes retrieved.
Out of these trials, MRC and Dutch gastric cancer trials gained the maximum popularity. These trials showed marginally better survival but that was not statistically significant. Probably, postoperative increased morbidity and mortality was related to partial pancreatectomy and splenectomy. Japanese continued insisting on better outcome with D2 gastrectomy and found a way to decrease morbidity and mortality by preserving spleen and pancreas without compromising lymphadenectomy.This concept was later validated by single institution RCT from Chile, (Csendes et al) which showed no difference in the morbidity and mortality in both the arms.
The JCOG is conducting a multi-institutional RCT comparing D2 dissection with or splenectomy for patients with proximal gastric cancer.
There is an evolving consensus that splenectomy should be performed only in case with intraoperative evidence of direct tumour extension in to spleen or when primary tumour is located in the proximal stomach along the greater curvature. Partial pancreatectomy should be performed only in cases of direct tumour extension to the pancreas.
We believe that D2 gastrectomy can provide a better oncological outcome over D1 gasterctomy and opt for splenctomy if tumour is involving the proximal stomach.
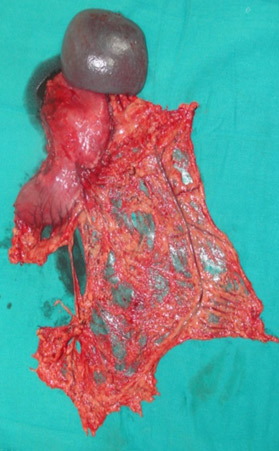
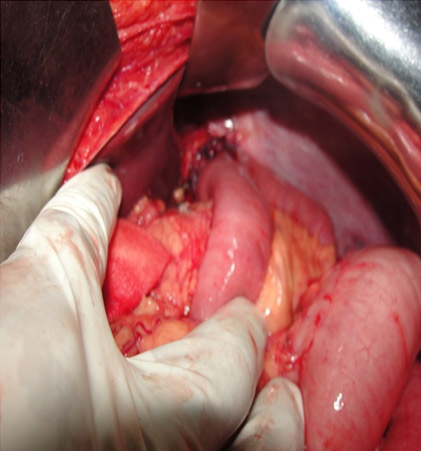
In the given case, signet ring cell carcinoma was involving the whole stomach. D2 gastrectomy and Roux en Y loop Oesophagojejunostomy has been performed. Patient recovered uneventfully and is on follow up.
For further information call :
DHARAMSHILA HOSPITAL AND RESEARCH CENTRE
Dharamshila Marg, Vasundhara Enclave,
Delhi – 110 096
Ph. 43066666, 43066571, 22618572
Fax No. 22617770, 22619033
E-mail : [email protected]
Website : www.thedhrc.org




