Dr. Suparno Chakrabarti,
MD (PGIMER, Chandigarh), MD (University of Birmingham, UK), FRCPath (UK)
Program Director, Department of BMT & Hematology,
Dharamshila Hospital And Research Centre, New Delhi
What is blood and marrow transplantation (BMT)?
Bone marrow transplantation (BMT) is a procedure in which healthy cells are transplanted in a patient’s body to replace damaged / diseased bone marrow.
BMT is used to treat patients with a variety of malignant (cancerous) and nonmalignant (noncancerous) diseases, including:
For the transplant, the stem cells can be collected from the body of the patient (Autologous Transplantation) after he / she has been treated, or from a donor (Allogeneic Transplantation). The procedure is termed as Syngeneic if the cells are collected from an identical twin. Other sources of healthy stem cells include matched and unrelated donors (MUD) or a cord blood transplant using stem cells collected from the blood of a newborn’s umbilical cord (from volunteer registries or Public Cord Blood Banks).
What is haploidentical BMT?
Haploidentical BMT is a procedure in which related donors, who don’t fully match the recipient may be considered for the bone marrow transplant.
Parents, children and 90% of our siblings are likely to qualify as donors in this procedure. However, the doctors will look into the general condition of the patient, nature of the disease, presence / absence of certain cell types and receptors in the patient and donor, and presence / absence of anti-cancer cells in the donor in order to decide whether an intended donor qualifies for donating
Why do we need a centre for haploidentical BMT?
In Delhi and NCR, we have six private and two state-owned BMT centres. We have over 40 centres across the country. So why then we required one more centre at DHRC? Because every year more than over 30,000 patients in our country need a BMT, but only about 1,000 transplants, actually take place (as per Indian Stem Cell Transplant Registry).
If all the centres across the country perform 4 transplants per month, the need would be largely met. However, BMT is dependent on availability of HLA matched donors from the family, which is available to only 20% of the patients by simple law of inheritance.
In Europe, USA and Japan, patients and their families meet their needs largely through Volunteer Unrelated Donor Registries which currently boast of 20 million donors. In India, however, these registries are in their infancy and the chance of finding a match from the foreign registries is less than 10%. Also, the cost of procuring the blood or marrow products from Europe or USA ranges from 10,000-30,000 USD. Similar transplants can be performed from unrelated cord blood units at a similar cost, but the procedure is more challenging. In such a scenario, a haploidentical BMT centre seems to be a logical option – because it has the potential to create an expanded pool of donors.
We started the first Haploidentical BMT program in India and Dr. Sarita Jaiswal joined the program after a year. The program was supported by Prof Paul O’Donnell from Fred Hutchinson Cancer Research Centre, Seattle, and Prof Franco Aversa, University of Perugia and Parma in Italy. Till now, we have performed more than 30 haploidentical transplants.
Protective isolation into clean rooms
BMT patients need ultra clean environments. They have low immunity levels and thus are at a greater risk of catching infections easily that might turn life-threatening.
We, at Dharamshila Cancer Hospital and Research Centre, put our patients in BMT Clean Rooms. These rooms are designed as per international standard “Class 100 for clean rooms” which is equivalent to ISO class 7.
Particle count in these rooms is maintained below 1000 by strictly following the specifications for HVAC systems, building design, building materials, treatment of water and by adhering to strict protocol for maintaining a totally germ free environment.
Total Body Irradiation (TBI)
It is a form of radiotherapy that is often used as a part of the preparative regimen for bone marrow transplantation. However, it often results in serious long term toxicities. To tackle this, we, at DHRC, employ VMAT technology that allows us to target the entire bone marrow at much higher doses without exposing other organs such as heart, lungs, liver or kidneys to the detrimental effect of radiation.
We also have the best and the latest diagnostic tools to identify donors for fully HLA Matched family donor and half matched family donor, and to preserve the donated stem cells. Our lab facilities include:
• Magnetic Separation of Cells using MACS Technology
• Long term cryopreservation of stem cells at -1960C liquid nitrogen freezer in vapour phase
• HLA typing, NK cell genotyping and CD34 + stem cell estimation
• Comprehensive donor selection for Haploidentical BMT, based on NK-KIR profile
• NK cell and mesenchymal cell therapy
• Molecular diagnosis for leukemia
• Flowcytometry based diagnostics for leukemia, lymphoma and Aplastic anemia
• Detection of Minimal Residual Disease (MRD)
• Conventional and Real Time PCR for Viral Pathogens.
Results and Accolades
We regularly perform Haploidentical BMT for all malignant and non-malignant diseases where BMT is indicated. We have transplanted 61 patients from Haploidentical family donors since 2010 and notably, 30 of those took place in the last 18 months.
The indications for BMT include Acute Leukemia, Lymphoma, Aplastic Anemia, Thalassemia and Sickle Cell Anemia. The success rate in terms of engraftment is 100% and survival has now touched 90% for all diseases with a median follow-up of 285 days (90-651 days) (Figure1).
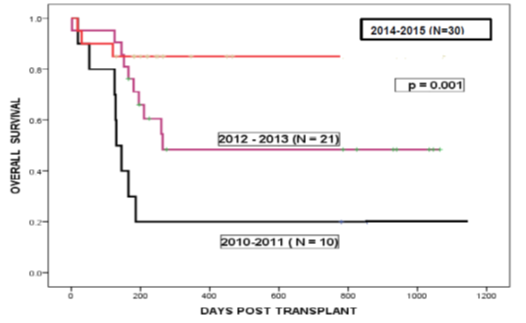
Figure1: Outcome of Haploidentical BMT over the last 5 years. The red line shows the overall survival of 30 patients who underwent Haploidentical BMT at DHRC during 2014-2015.
Dr. Sarita Jaiswal (trained under Prof. Franco Aversa from Italy), a pioneer of Haploidentical BMT, Prof Aversa and other specialists came together to build a whole new approach to Haploidentical BMT using Clinimacs based manipulation of graft. This new approach to BMT has drastically reduced the rate of complications and mortality experienced earlier. Dr Sarita also had the privilege of training in BMT at the largest BMT centre of the world, i.e., Fred Hutchinson Cancer Research Centre, Seattle. The experience at University of Parma under Prof Aversa and at Seattle inspired Dr Sarita to develop the Haploidentical BMT program in India to make the procedure affordable and available to all.
Later on, the study conducted by Dr Sarita and her team (on 41 patients with leukemia and aplastic anemia) was selected for an oral presentation at the Annual BMT meeting of American Society of Blood and Marrow Transplantation (ASBMT) and Centre for International Bone Marrow Transplant Registry (CIBMTR) in February 2015 at San Diego, USA. Dr Sarita Jaiswal presented the study of Haploidentical BMT demonstrating improving outcome in both leukemia and aplastic anemia over the last 4 years. In her presentation, she shared the data on how they selected anticancer cells from the donors and gave them to the patients after Haploidentical transplantation procedures (for more on this, read here. Dr Sarita Jaiswal now leads the Haploidentical BMT program at Dharamshila Hospital, New Delhi.




