
Departments
Radiation Oncology
Radiation Oncology
External radiotherapy
Volumetric Modulated Arc Therapy (VMAT)
Image Guided Radiation Therapy (IGRT)
Intensity Modulated Radiation Therapy (IMRT)
Stereotactic Radiation Therapy (SRT)
Stereotactic Radio Surgery (SRS)
Stereotactic Body Radiation Therapy (SBRT)
Three-Dimensional Conformal Radiation Therapy (3-D CRT)
Respiratory Gating
Internal Radiotherapy
Remote After Loading High Dose Rate Brachytherapy (HDR Brachytherapy)
Medical Oncology
Medical Oncology
Chemotherapy
Hormonal Therapy
Immunotherapy / Biological Therapy
Targeted Therapy
Neutropenic Care
Nutritional Therapy
Haemato Oncology
Surgical Oncology
Surgical Oncology
Neuro Oncology
Head and Neck Oncology
Breast Oncology
Thoracic Oncology
Gynaec Oncology
Cosmetic and Reconstructive Surgery
G. I. Oncology
Uro Oncology
Musculo-skeletal Oncology
Laparoscopic/ Minimally Invasive surgery
Gynaec Oncology
Gynaec Oncology
Cancer of Cervix
Cancer of Ovary and Fallopian Tube
Cancer of Uterine Cavity
Cancer of Vulva
Cancer of vagina
Cancer of Persistent Gestational Trophoblastic Tumor (GTNs)
Anesthesiology & Critical
Radiology & Imaging
Pathology & Transfusion
Pathology & Transfusion
Histopathology
Cytopathology
Haematology
Biochemistry
Serology
Clinical Pathology
Microbiology
Transfusion Medicine
Emergency Services
Nursing Services
Our Doctors

- Featured Doctors in Popular Specialties.... ........ Read more
Diseases Treated
The following types of cancers are managed under sub-speciality of gynecology Oncology:
High risk Women: low socioeconomic status; women with poor personal hygiene, multiparity, early age of sexual intercourse, multiple sexual partners. Smoking, folate deficiency and other associated vulvo-vaginal infections (herpes simplex), HIV infections, immuno-deficiencies conditions are cofactors.
Causative Agent: The main cause of cervical cancer is human papilloma virus (HPV). It is passed from one person to another during sex. These viral infections clears off in most by itself, but persist in some due to unknown reasons and results into cancer.
Sign & Symptoms
Abnormal vaginal bleeding
Post coital bleeding
Persistent discharge Per vaginum
In neglected cases (very late stages: stage IV):- persistent bleeding or bowel and bladder pressure symptoms, incontinence of urine or faeces, severe backache/bone pains.
Stage of cervix cancer
Pre-malignant stage: CIN2/3
Pre-invasive stage( 0 stage): carcinoma in situ
Stage I-IV: depending upon increasing spread of disease tumor is classified into higher stages
Diagnostic test
Early stage: Colposcopy directed biopsy( OPD procedure)
Late stages: Direct Punch biopsy (OPD Procedure)
Treatment
Very early stages( early micro-invasion): LEEP, Cold or laser knife conisation, simple hysterectomy
Late early Stages (stage IA2, IB1,IB2 , IIA): Surgical treatment in form of Radical hysterectomy cancer; that is removal of cervix with adjacent tissues and draining lymph nodes ( Wertheim's hysterectomy with retroperitoneal lymph node dissection) with or without adjuvant tailored pelvic radiotherapy. Late stages( Stage IIB to III B): Radiotherapy with concurrent chemotherapy
Very late stages (Stage IV): Palliative RT
Prognosis
Stage IA : 95-98%
Stage IB : 79-90%
Stage II : 70-77%
Stage III : 45%
StageIV : 12-22%
Prevention: regular Pap's smear in reproductive age group women after marriage, HPV DNA testing, if suspicious for abnormality is found colposcopy and directed biopsy is done. Recently introduced HPV vaccine is FDA approved for school going girls (9-15yrs) for prevention of cancer cervix, but it is not to be replaced by regular Pap's smear.
Causative Agent: The main cause of cervical cancer is human papilloma virus (HPV). It is passed from one person to another during sex. These viral infections clears off in most by itself, but persist in some due to unknown reasons and results into cancer.
Sign & Symptoms
Abnormal vaginal bleeding
Post coital bleeding
Persistent discharge Per vaginum
In neglected cases (very late stages: stage IV):- persistent bleeding or bowel and bladder pressure symptoms, incontinence of urine or faeces, severe backache/bone pains.
Stage of cervix cancer
Pre-malignant stage: CIN2/3
Pre-invasive stage( 0 stage): carcinoma in situ
Stage I-IV: depending upon increasing spread of disease tumor is classified into higher stages
Diagnostic test
Early stage: Colposcopy directed biopsy( OPD procedure)
Late stages: Direct Punch biopsy (OPD Procedure)
Treatment
Very early stages( early micro-invasion): LEEP, Cold or laser knife conisation, simple hysterectomy
Late early Stages (stage IA2, IB1,IB2 , IIA): Surgical treatment in form of Radical hysterectomy cancer; that is removal of cervix with adjacent tissues and draining lymph nodes ( Wertheim's hysterectomy with retroperitoneal lymph node dissection) with or without adjuvant tailored pelvic radiotherapy. Late stages( Stage IIB to III B): Radiotherapy with concurrent chemotherapy
Very late stages (Stage IV): Palliative RT
Prognosis
Stage IA : 95-98%
Stage IB : 79-90%
Stage II : 70-77%
Stage III : 45%
StageIV : 12-22%
Prevention: regular Pap's smear in reproductive age group women after marriage, HPV DNA testing, if suspicious for abnormality is found colposcopy and directed biopsy is done. Recently introduced HPV vaccine is FDA approved for school going girls (9-15yrs) for prevention of cancer cervix, but it is not to be replaced by regular Pap's smear.
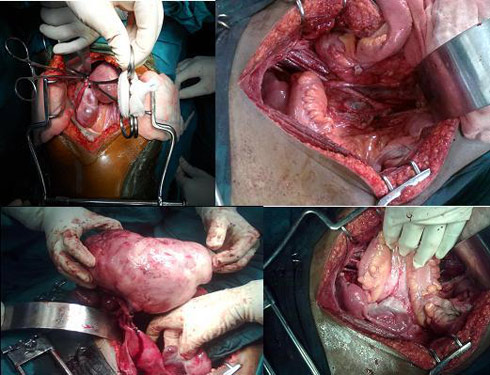
Photograph of Specimen removed of Radical Hysterectomy with pelvic Lymph node dissection

Classification: mainly these are of 4 types as follow:-
Stage I : cancer is limited to the ovaries
Stage II : cancer is involving one or both ovaries, but extends to pelvis
Stage III : cancer is microscopically or gross spread outside the true pelvis into the abdomen; on omentum, liver surface, small or large bowel or peritoneum
Stage IV : cancer spread to distant sites, including pleural effusion with positive cytologic test or parenchymal liver metastasis equals stage IV
Etiopathogenesis
Prognosis in ovarian cancers:
- Epithelial ovarian cancers (85-90%)
- Germ cell Ovarian cancers (10-15%)
- Sex-cord stromal tumors
- Kruckenberg or other metastatic or others rare tumors
Stage I : cancer is limited to the ovaries
Stage II : cancer is involving one or both ovaries, but extends to pelvis
Stage III : cancer is microscopically or gross spread outside the true pelvis into the abdomen; on omentum, liver surface, small or large bowel or peritoneum
Stage IV : cancer spread to distant sites, including pleural effusion with positive cytologic test or parenchymal liver metastasis equals stage IV
Etiopathogenesis
- Exact causative agent and etio-pathogenesis is still not known
- Certain women are high risk due genetic predisposition. History of ovarian, breast or colon in more than one, 1st or 2nd degree blood relatives on maternal or paternal side predisposes for it( HBOS,HNPCC/LynchII)
Early stage
Asymptomatic except some vague complaints of dyspepsia or feeling of fullness in lower abdomenLate stages
may manifest with following sign or symptoms:- Pain in abdomen
- Weight loss
- Loss of appetite, early satiety, difficulty to eat, dyspepsia, bloating sensation or fullness of abdomen
- frequency of urination
- In advanced metastatic stage its signs like abdominal distension, pain in abdomen, hard mass in pelvis or abdomen, ascites , pleural effusion etc
For early detection of ovarian cancers
- Annual pelvic or vaginal examination by Gynecologist
- Annual pelvic Sonography
To confirm the diagnosis
- Sonography or CT Scans
- various tumor markers in blood:CA125,CEA, BHCG,AFP,LDH
- fine needle aspiration cytology (advanced stages)
- Ovarian cancers are mainly treated with surgery with adjuvant chemotherapy.
- Role of surgery: to diagnose and to stage (staging laparotomy) in early stages (I&II); while in late stages(III &IV), it is done to de-bulk the tumor load followed by tumor left over cells to be taken care of by chemotherapy drugs.
- In few selected cases, where upfront surgery can not be done for various reasons, chemotherapy (neo-adjuvant) is given to decrease the tumor load followed by surgery
- Fertility Preservation surgeries are done in suitable localized tumors, if women is desirous for it with due risk of recurrence explained to them. They are kept under close observation till the time completion of surgery is done
Prognosis in ovarian cancers:
- Epithelial ovarian cancers: early stages : around 90%
- Overall prognosis: around 50%
- Germ cell tumors are generally associated with high cure rate and good survival
- Sex cord tumors though have good prognosis , but known for late recurrences
Incidence
Predisposing high risk Factors
Presenting Features
Staging of Uterine Cancers
Diagnosis
Treatment
Prognosis
- It is commonest genital tract malignancy among women of in western countries. In United States about 41,200 new cases registered every year.
- Its incidence in India the is on the rise mainly because of the changes in the lifestyle & obesity.
- In population based cancer registry of Delhi, the incidence of endometrial cancer is 4.3/ 100,000 women per year (ICMR).
- >70% of cases, are confined to uterus at time of diagnosis
Predisposing high risk Factors
- Most uterine cancers develop at age >50years , but 10% of them are in <40 yrs of age.
- Exposure to unopposed estrogen; ERT, anovulatory cycles/infertility, obesity, estrogen secreting tumors.
- Tamoxifen exposure increases risk to 2-3 folds.
- Family history of uterine, breast, ovarian or colorectal cancers.
- Occasionally may develop post radiation for cancer cervix.
Presenting Features
- Abnormal vaginal bleeding in 90% cases, especially if in postmenopausal women
- Abnormal inter-menstrual or heavy prolonged peri-menopausal bleeding
- Some may present with purulent vaginal discharge
- High index of suspicion is necessary to diagnose it in young women, who has history of PCOD/ anovulatory cycles
- Abnormality in pap smear
Staging of Uterine Cancers
- Stage I: In this stage the cancer is limited to the uterus
- Stage II: In this stage the cancer spread to the cervix area of the uterus
- Stage III: In this stage, cancer reached an advanced phase but it is still located only in the pelvis
- Stage IV: In this stage, the cancer spreads massively to the entire pelvic cavity or affected distant organs and areas
Diagnosis
- Pelvic sonography
- Endometrial sampling by EB or D&C
Treatment
- Surgery: Staging laparotomy:- Total hysterectomy with BSO with lymph node dissection upto para-aortic lymph nodes, followed by adjuvant tailored radiotherapy. Sometimes hormonal therapy or chemotherapy may also be required.
Prognosis
- 5 year survival rate varies with histo-pathological type of tumor
- Endometriod type variety of uterus is highly treatable cancer in early stages and fortunately most cases(>70% ) are diagnosed, when confined is still to uterus( Stage I ).
- Survival rates are lower in other varieties like uterine papillary serous or sarcomatous or mixed mullerian types
Incidence: it accounts for 4% of genital tract malignancies.
Aetiology: No specific etiological factor has been found in vulvar cancers, though many cases are associated / preceded by vulvar dystrophies and VIN. Some association has been found with HPV infection, specially in young women.
Symptoms& signs
Stage 0 (Carcinoma in Situ): Abnormal cells confined to skin
Stage I: cancer localized to vulva only or in the vulva and perineum, but size < 2cms
Stage II: cancer in vulva and perineum of size >2cms
Stage III: cancer is of any size, but spread is present to unilateral groin nodes or to lower third vagina / urethra or anus
Stage IV: spread to bilateral groin nodes /upper part of urethra/bladder/rectum/pelvic bone/ distant metastasis
Treatment
Prognosis: with appropriate management 5 year survival rate in operable cases is generally good in range of 70%. The stage wise prognosis is 98%,85%, 74% and 31% in stage I,II, III and IV respectively. Positive groin lymph nodes and their number worsen the prognosis.
VIN (premalignant stage of vulvar cancers): Colposcopy has a role in detecting it in premalignant stages (Vulvar intraepithelial Neoplasia) before it gets transformed into fully malignant form. VIN can be treated with very simple procedures like laser excision/ knife excision. Some other predisposing conditions need regular biopsies and require prolonged local steroid ointment and regular follow up.
Aetiology: No specific etiological factor has been found in vulvar cancers, though many cases are associated / preceded by vulvar dystrophies and VIN. Some association has been found with HPV infection, specially in young women.
Symptoms& signs
- Itching at vulva (labia majora, minora, fourchette, periurethral region, cliral or peri-clitoral region)
- change in pigmentation of skin and mucosa in vulva region
- mass in vulvar region
- rarely bleeding or infected fungating large tumors in vulvar region in late neglected cases.
Stage 0 (Carcinoma in Situ): Abnormal cells confined to skin
Stage I: cancer localized to vulva only or in the vulva and perineum, but size < 2cms
Stage II: cancer in vulva and perineum of size >2cms
Stage III: cancer is of any size, but spread is present to unilateral groin nodes or to lower third vagina / urethra or anus
Stage IV: spread to bilateral groin nodes /upper part of urethra/bladder/rectum/pelvic bone/ distant metastasis
Treatment
Role of Surgery in management of vulvar cancers
- There had been a paradigm shift in vulvar cancer management with individualization, multidisciplinary treatment with stress on vulvar conservation surgeries in localized vulvar cancers.
- Primarily patient is treated with conservative or radical surgeries
- Groin node dissection is done along with vulvar surgery, followed by adjuvant radiotherapy if indicated by final histopathology report.
Role of radiotherapy in management of vulvar cancers
- After surgery to prevent local recurrence , if margins are close
- As primary treatment, in small primary lesions of clitoral or para-clitoral in young women
- In cases of microscopic or macroscopic groin node metastasis
- If lesion is too close to anal sphincter or involving the upper urethra or vagina
Prognosis: with appropriate management 5 year survival rate in operable cases is generally good in range of 70%. The stage wise prognosis is 98%,85%, 74% and 31% in stage I,II, III and IV respectively. Positive groin lymph nodes and their number worsen the prognosis.
VIN (premalignant stage of vulvar cancers): Colposcopy has a role in detecting it in premalignant stages (Vulvar intraepithelial Neoplasia) before it gets transformed into fully malignant form. VIN can be treated with very simple procedures like laser excision/ knife excision. Some other predisposing conditions need regular biopsies and require prolonged local steroid ointment and regular follow up.
Cancer of Vagina occur in vagina and commonly it is of squamous cell carcinoma , and less commonly it is adenocarcinoma variety . In younger age group , though rare sarcoma botroides, germ cell tumor or rhabdo myosarcoma varieties may occur.
Risk Factors
Stage 0 (Carcinoma in Situ): when cancer is localized to epithelial lining of vagina
Stage I: Cancer breaches the basement membrane of epithelium, but localized to vagina only
Stage II: cancer spread to surrounding tissues around vagina
Stage III: cancer spread to lymph nodes in pelvis or groin or it reaches up to pelvic walls
Stage IV: Distant metastasis
Sign & symptoms
Stage 0 Vaginal Cancer (carcinoma in situ):
Stage I : Vaginectomy or , hysterectomy, and lymphadenectomy. This may be followed by vaginal reconstruction and/or radiation therapy. Radiotherapy also gives equally good results.
Stage II: either only radiotherapy or surgery (Vaginectomy or pelvic exenteration) with or without radiation therapy.
Stage III: in advanced stages radiotherapy gives better results, in stage IV A & B, the aim is palliative treatment, to give symptomatic relief and improve the quality of life. Chemotherapy may also be given. Patient can participate in clinical trial of chemotherapy and / or radio sensitizers.
Risk Factors
- > 60 years age
- HPV infection
- women exposed to DES( Diethyl stilbesterole)in utero
Stage 0 (Carcinoma in Situ): when cancer is localized to epithelial lining of vagina
Stage I: Cancer breaches the basement membrane of epithelium, but localized to vagina only
Stage II: cancer spread to surrounding tissues around vagina
Stage III: cancer spread to lymph nodes in pelvis or groin or it reaches up to pelvic walls
Stage IV: Distant metastasis
Sign & symptoms
- bleeding per vaginum
- white discharge per vaginum
- in advanced cases : pain in lower abdomen, backache, pain radiating to legs, urinary or fecal incontinence
- History & Examination
- Pap's Smear
- Colposcopy
- Biopsy
- X Ray chest , CT Scan, MRI, Lymphangiography, Cytoscopy, Ureteroscopy, Proctoscopy help in planning of treatment
Stage 0 Vaginal Cancer (carcinoma in situ):
- Wide local excision, with or without a skin graft
- Partial or total vaginectomy, with or without a skin gzaft.
- Topical chemotherapy or Laser surgery or internal radiation therapy.
- Internal radiation therapy, with or without external radiation therapy to lymph nodes or large tumors
- Wide local excision or vaginectomy with vaginal reconstruction. Radiation therapy may be given after the surgery
- Vaginectomy and lymphadenectomy, with or without vaginal reconstruction. Radiation therapy may be given after the surgery.
Stage I : Vaginectomy or , hysterectomy, and lymphadenectomy. This may be followed by vaginal reconstruction and/or radiation therapy. Radiotherapy also gives equally good results.
Stage II: either only radiotherapy or surgery (Vaginectomy or pelvic exenteration) with or without radiation therapy.
Stage III: in advanced stages radiotherapy gives better results, in stage IV A & B, the aim is palliative treatment, to give symptomatic relief and improve the quality of life. Chemotherapy may also be given. Patient can participate in clinical trial of chemotherapy and / or radio sensitizers.
Persistent GTN tumor include spectrum of disease and are curable malignancies with good prognosis. But, most cases of persistent Gestational trophoblastic tumors are neglected and report for treatment when already tumor has metastasized in different organs like into lung, brain, vagina or pelvic structures. Persistent GTNs are one of the gynecology oncologic emergencies.
Stages of GTN
Symptoms of Persistent GTN
Follow up Follow up is done with serum b HCG levels and clinical examination . with USG whenever it is indicated
In Stage I, II, III: weekly follow up 3 weeks & monthly for 12 months
Prognosis: GTN is a curable malignancy and has good prognosis with appropriate timely management with surgery and chemotherapy.
Stages of GTN
- Non- metastatic: disease confined to uterus
- Metastatic: Disease spread outside the uterus
Symptoms of Persistent GTN
- Persistent vaginal bleeding precede by history of abortion, full term pregnancy or vesicular mole.
- Persistently raised B HCG after evacuation of vesicular mole.
- Pulmonary metastasis with breathlessness.
- Rarely haemo-peritoneum due to involvement of uterine artery.
- Late neglected cases with brain metastasis may present with epileptic fits, comma or violent behaviour.
Role of Surgery
- Stage I : If patient no longer wishes to preserve fertility ,hysterectomy with adjuvant chemotherapy should be performed
- Hysterectomy is done in all cases of placental site trophoblastic tumors
- Surgery is done in form of uterine artery or internal iliac ligation in cases of uncontrolled bleeding, who are desirous to preserve fertility. If facility available uterine artery embolization may also be tried in these cases.
- Thoracotomy rarely required excising persistent lung metastasis even after chemotherapy.
Role of chemotherapy
Low risk GTN(WHO Score<7) are treated with single agent Methotraxate or Actinomycin D, while and high risk GTN ( Score >7)are treated with multi-agent EMA-CO with or without brain radiotherapy and intrathecal methotraxate.Follow up Follow up is done with serum b HCG levels and clinical examination . with USG whenever it is indicated
In Stage I, II, III: weekly follow up 3 weeks & monthly for 12 months
- Weekly bHCG x3 consecutive weeks
- Monthly BHCG X 12 months
- Effective contraception for period of hormonal follow up
Prognosis: GTN is a curable malignancy and has good prognosis with appropriate timely management with surgery and chemotherapy.
Cancer of cervix, ovary, uterus and vagina together are responsible for around one quarter of new female cancer cases registered in most cancer registries in India.
- Diseases Treated
- Infrastructure
- Information
- Research & Training
Follow us on